Cardiotoxicity of PR-171 (Carfilzomib): A Systematic Review and Meta-Analysis of Clinical Safety
Abstract
The potent antitumor activity of PR-171 (Carfilzomib) is a second generation proteasome inhibitor, abbreviated as PI, that is approved for patients with relapsed or refractory multiple myeloma, abbreviated as RRMM, who failed one or more prior lines of therapy. A systematic review of PR-171 literature with meta-analysis was performed to determine cumulative incidence of cardiotoxicity. After the literature search, a total of 29 eligible phase I/II, phase II and phase III clinical trials which used PR-171 were included. The cumulative incidence and overall odds ratios, abbreviated as OR, were calculated with random effect model using R software with metaphor package. A total of 4164 patients with various malignancies were included. The overall estimated cumulative incidence of cardiotoxicity was 8.68% and 4.92%, respectively, for all grade and high grade which is grade 3 or higher toxicity, which seems higher than other PIs. Compared to control group, the odds of developing cardiotoxicity due to PR-171 was significantly higher with OR of 2.03 with 95% CI at 1.19 to 3.46 and p equals 0.010 and 2.04 with 95% CI at 1.31 to 3.17 and p equals 0.002 for all grades and high grades, respectively. Concomitant immunomodulatory agents seem to increase the risk of cardiotoxicity with high grade cardiotoxicity at 6.45% and 4.34% with and without concomitant immunomodulatory agents, respectively, with p equals 0.033. There was no variation in the incidence of cardiotoxicity among newly diagnosed versus RRMM with p equals 0.38, and high versus standard dose PR-171 with p equals 0.86.
Key Terms and Abbreviations
The research involves numerous important scientific and medical terms and abbreviations. PR-171 is abbreviated as Carf. Multiple myeloma is abbreviated as MM. Relapsed or refractory multiple myeloma is abbreviated as RRMM. Newly diagnosed multiple myeloma is abbreviated as NDMM. Proteasome inhibitor is abbreviated as PI. Immunomodulators are abbreviated as IMiDs. Odds ratio is abbreviated as OR. Confidence interval is abbreviated as CI. Hypertension is abbreviated as HTN. Tumor necrosis factor alpha is abbreviated as TNF-alpha. Interleukin 6 is abbreviated as IL-6. Common Terminology Criteria for Adverse Events is abbreviated as CTCAE. Endothelial nitric oxide synthase is abbreviated as eNOS. Nitric oxide is abbreviated as NO. Congestive heart failure is abbreviated as CHF. Brain natriuretic peptide is abbreviated as BNP. Preferred Reporting Items for Systematic Reviews and Meta-Analysis is abbreviated as PRISMA. International Prospective Register for Systematic Reviews is abbreviated as PROSPERO. DerSimonian-Laird estimator is abbreviated as DL.
Introduction
Survival rates have improved recently in multiple myeloma patients due to the administration of the novel therapeutics such as proteasome inhibitors and immunomodulators. Bortezomib is first in class of PI, which is approved in the USA for the treatment of patients with MM and mantle cell lymphoma. It is modified dipeptidyl boronic acid PI, which reversibly inhibits the protease activity of 26S proteasome which is responsible for degradation of intracellular proteins through the ubiquitin proteasome pathway. Inhibition of proteasomal activity disrupts the cell signaling pathways which lead to apoptosis and ultimately cell death. PR-171, abbreviated as Carf, is the second generation PI that irreversibly inhibits 20S proteasome and is approved as a combination therapy with dexamethasone or with lenalidomide plus dexamethasone for the treatment of patients with relapsed or refractory MM who have received one to three lines of therapy and as a single agent for patients with RRMM who have received one or more lines of therapy. Multiple clinical trials have utilized Carf based regimens also in patients with newly diagnosed MM with promising results.
PIs have shown to be potently toxic to myocytes likely due to inhibition of proteasomal dependent sarcomeric protein turnover leading to apoptosis and cell death. One systematic review and meta-analysis showed the incidence of all grade and high grade cardiotoxicity associated with bortezomib was 3.8% and 2.3%. However, it also concluded that the use of bortezomib did not significantly increase the risk of all grade with OR 1.15 and 95% CI at 0.82 to 1.62 with p equals 0.41 and high grade with OR 1.13 and 95% CI at 0.58 to 2.24 with p equals 0.72 cardiotoxicity compared with patients treated with control medication. In Carf based regimens, most common adverse events reported of any grade included fatigue, anemia, nausea, dyspnea, thrombocytopenia, diarrhea, pyrexia and headache. The reported incidence of cardiotoxicity due to Carf in the clinical trials varies widely and there are also reports on cardiotoxicity in real life practice. These events can also lead to hospitalization, discontinuation of Carf and even death. One group analysis showed that among the patients who discontinued Carf for various reasons, 14.8% had cited an adverse event as the underlying reason for discontinuation and 4% discontinued due to a cardiac event. Even though the cardiotoxicity with Carf is relatively infrequent, it can have significant clinical implications and therefore with the increasing use of Carf, there is the need to better understand the toxicity profile of this novel agent. Based on published literature, it is hypothesized that the cardiotoxicity with Carf is more frequent than that seen with other PIs. So the aims of the study are to calculate cumulative incidence and risk of cardiotoxicity due to Carf by analyzing data available in published clinical trials. This study will help understand the cardiotoxicity associated with this important drug and help guide physicians using it in a real world practice.
Materials and Methods
Study Selection and Design
The selection and systematic review of trials were performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis statement. The protocol of the current meta-analysis was registered at the International Prospective Register for Systematic Reviews with registration number CRD42017067229.
Literature Search Strategy
Two investigators, which are CS and RB, conducted an independent literature search of PubMed, Web of Science, and clinical trial registry at http://clinicaltrials.gov. Abstracts from American Society of Clinical Oncology and American Society of Hematology conferences that took place since its inception to January 2017 were also searched. Key words used were carfilzomib, Kyprolis, PR-171, and cancer. Reference list of selected studies and other published systematic reviews were also searched separately to capture any relevant studies. Studies published prior to January 2017 were selected. In the case of multiple publications originating from a single trial or duplicate publications, only the most recent and updated report of the clinical trial were included.
Selection of Study and Data Extraction
The primary goal of the meta-analysis was to calculate the incidence of cardiotoxicity secondary to Carf and to estimate the risk of developing cardiotoxicity. Only prospective trials published prior to January 2017 and written in the English language were included. Studies were included if the participants were assigned to treatment with Carf alone or in combination with other agents. Only those studies were included which had sufficient information on cardiotoxicity. A total of 32 phase I studies were excluded due to variable doses of Carf and relatively small sample size. One phase III study was included which did not have information about the control arm yet.
Two investigators, which are CS and RB, independently conducted the data extraction from included studies, and any discrepancy between the two was resolved by consensus. These data include first author’s name, year of publication, phases of trials, underlying malignancy and histology, the trial number when available, a total number of enrolled patients, the median age of patients, dose of Carf, treatment regimen, adverse cardiac events of interest and type of events. As for the adverse events, studies recorded the adverse events as all grade or high grade based on the Common Terminology Criteria for Adverse Events version 2, 3 or 4, which is widely accepted in clinical trials. Adverse cardiac events reported were acute coronary syndrome, acute left or right ventricular failure, acute myocardial infarction, angina pectoris, various arrhythmias, cardiac arrest, cardiac failure and cardiomyopathy. Events were not included in calculations whenever it was specifically reported in the article that the events were not secondary to the drug of interest. Similarly, another toxicity that was associated with the use of Carf which is arterial hypertension was also recorded and analyzed.
Embracing a holistic approach to the products we enjoy involves understanding both the artisanal techniques behind fermentation and the broader environmental systems that support modern production. For those curious about the science of preservation, the CX-5461 with Foire aux Questions : Les légumes lacto fermentés – Les Jarres Crues offers a deep dive into traditional biological processes. In our quest for sustainable operations, it is also vital to evaluate our global footprint by Comparing Energy Costs of Nuclear, Pidnarulex,Coal, Gas, Wind and Solar. By fostering strong connections through our network of Nab-Paclitaxel | Nos Partenaires – Aliments lacto-fermentés – Les Jarres Crues, we ensure that every step of our journey reflects a commitment to quality and responsible innovation.
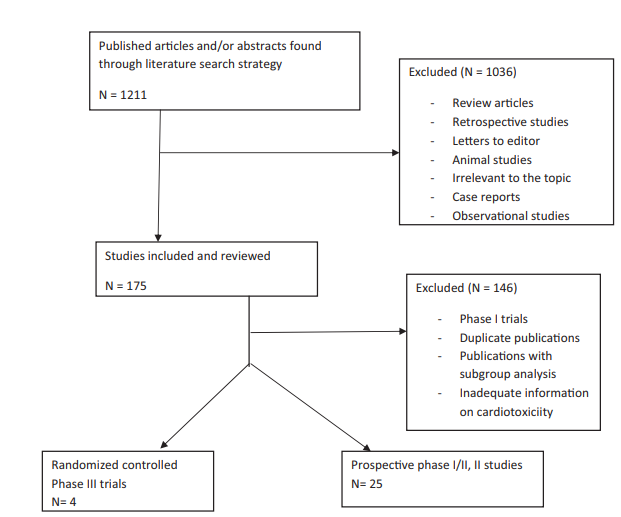
Figure 1. Process of selection of clinical trials for meta-analysis.
Subgroup Analysis
To evaluate the effect of various risk factors onto the incidence of cardiotoxicity and HTN, a meta-analysis of various subgroups was performed. First, it was hypothesized that patients with RRMM would have had previous exposure to other chemotherapeutic agents in various combinations and therefore more likely to suffer toxicities. To test the hypothesis, MM studies were divided into two groups: those who had NDMM patients and those who had RRMM patients. Second, in order to analyze the difference in the incidence of cardiotoxicity based on the dose of Carf used, studies were divided into two groups: standard dose at 27 mg/m2 or less and high dose such as 36, 45, 56, 70, 88 mg/m2. From the included studies, Berenson and colleagues and Bringhen S and colleagues used once weekly dosing of Carf while others have used twice weekly dosing.
In a third analysis, the incidence of cardiotoxicity was calculated based on the regimen used such as Carf monotherapy versus combination with other agents. Finally, the incidence rates were also calculated and compared based on the concomitant use of IMiDs with Carf.
Study Quality and Statistical Analysis
Study quality and risk of bias was assessed using the Cochrane Collaboration’s tools. The cumulative incidence of toxicity and its 95% confidence interval were derived based on the reported number of patients who developed adverse events of interest out of the number of enrolled patients received Carf in respective studies. From studies with data available for the control group, summary odds ratio by DerSimonian-Laird estimator and its 95% confidence interval were calculated. All tests with p value less than 0.05 were considered statistically significant. The heterogeneity between studies was assessed by I-squared statistic test, where values less than 25%, 25% to 50% and greater than 50% were considered as a low, moderate and high degree of heterogeneity, respectively. The publication bias was assessed by visual inspection of the funnel plots and Egger’s test. All statistics were calculated using R software with metafor package.
Results
Study Characteristics
Based on the search criteria, 29 prospective studies of Carf enrolling a total of 4164 patients were identified. This includes 2036 patients from controlled trials with 1017 cases and 1019 controls. Age of patients included in studies ranged between 27 and 91 years and the median age of patients ranged between 58 and 72 years. Out of 29 studies, 27 studies enrolled patients with Multiple Myeloma (MM), which included NDMM, smoldering myeloma and RRMM. In one study, patients with Waldenstrom macroglobulinemia were included. Moreover, one study enrolled patient with various solid tumor such as small cell lung, nonsmall cell lung, renal and ovarian cancers.
Cumulative Incidence of Cardiotoxicity and HTN
Using a random effect model with DL, the cumulative incidence of all grade cardiotoxicity among 2660 patients from 23 studies was 8.68% with 95% CI at 6.13% to 11.59%. For high grade cardiotoxicity, a total of 2808 patients were included from 28 trials. Similarly, using the same model, the cumulative incidence of high grade cardiotoxicity was 4.92% with 95% CI at 3.91% to 6.02%. Reported cardiac toxic events include congestive heart failure, ischemic heart disease, arrhythmias and even cardiorespiratory arrest. Arrhythmias included atrial fibrillation, conduction abnormalities, ventricular arrhythmias, supra-ventricular tachycardia and other. The incidence of mortality associated with cardiotoxic events was 0.91% with 95% CI at 0.49% to 1.43%.
For all grade HTN, a total of 1905 patients were included from 14 different trials. The cumulative incidence of all grade HTN from these studies was 11.53% with 95% CI at 7.69% to 15.97%. For high grade HTN, the cumulative incidence of high grade HTN was 4.60% with 95% CI at 2.42% to 7.33% among a total of 1981 patients were included from 14 trials.
Estimated Overall Odds Ratio of Cardiotoxicity and HTN
There were three phase III studies in which comparison was made between Carf and control arms. To calculate the contribution of Carf into the development of the adverse events, random effect model with DL was performed to calculate the overall OR from these three trials. There were a total of 2036 patients. Estimated overall OR of all grade cardiotoxicity between Carf and control was 2.03 with 95% CI at 1.19 to 3.46 and p equals 0.010. Similarly, the OR of high grade cardiotoxicity was 2.04 with 95% CI at 1.31 to 3.17 and p equals 0.002. The overall OR of all grade HTN between Carf and control was 2.93 with 95% CI at 2.21 to 3.89 and p less than 0.0001. Similarly, the overall OR of high grade HTN was 3.33 with 95% CI at 1.98 to 5.60 and p less than 0.0001. These findings suggest Carf significantly increases the risk of developing HTN in cancer patients.
Subgroup Analysis for Cardiotoxicity and HTN
Various different factors can affect the incidence of cardiotoxicity and so a meta-analysis of multiple subgroups was performed. No difference in the incidence of all grade with p equals 0.38 and high grade with p equals 0.46 cardiotoxicity between NDMM and RRMM groups was found. It was surprising to see that the high dose of Carf did not change the incidence of all grade with p equals 0.63 or high grade with p equals 0.86 cardiotoxicity when compared to studies with a standard dose of Carf. Similarly, the incidence of all grade with p equals 0.06 and high grade with p equals 0.10 cardiotoxicity was not significantly different when Carf used alone or in combination. However, concomitant use of IMiDs significantly increased the incidence of all grade with p equals 0.006 and high grade cardiotoxicity with p equals 0.033.
As opposed to cardiotoxicity, high dose Carf was associated with higher incidence of high grade HTN with p equals 0.032 while not affecting all grade HTN with p equals 0.89. The incidence of high grade HTN with high dose was 6.40% with 95% CI at 3.50% to 9.99%, while it was 2.38% with 95% CI at 0.58% to 5.09% with standard dose Carf. But this difference was not significant for all grade HTN. A trend toward significant difference in the incidence of all grade HTN between RRMM group and NDMM group was found at 13.64% versus 7.47% with p equals 0.06, while the incidence of high grade HTN between RRMM and NDMM group was not statistically different with p equals 0.42. No significant difference in the incidence of all grade with p equals 0.27 and high grade HTN with p equals 0.59 was found when Carf used alone or in combination. Similarly, the incidence of all grade with p equals 0.98 and high grade with p equals 0.92 HTN was not significantly different when IMiDs were used concomitantly with Carf.
Publication Bias
No publication bias was detected by visual inspection of funnel plot and by Egger’s test for all grade cardiotoxicity with p equals 0.200 and high grade cardiotoxicity with p equals 0.762.
Discussion
Cardiotoxicity Incidence and Comparison
This is to the best of knowledge the first analysis incorporating a large pool of 29 clinical trials with 4164 patients investigating cardiotoxicity and HTN potential side effects of Carf. By analyzing published data of these clinical trials, it was found the incidence of all grade cardiotoxicity was 8.68% and high grade cardiotoxicity was 4.92%. Although a direct comparison cannot be made, the overall incidence of cardiotoxicity seems higher with Carf than that reported with bortezomib based regimens in trials which showed 3.8% and 2.3%, respectively, for all grade and high grade cardiotoxicity. A head to head comparison between Carf and bortezomib based regimens was done in the ENDEAVOR trial and it also showed a higher incidence of cardiotoxicity in Carf arm compared to bortezomib arm at 10.7% versus 4.7%. Moreover, it was also identified that the Carf significantly increases the risk of developing all grade with p equals 0.010 and high grade cardiotoxicity with p equals 0.002. Furthermore, Carf also significantly increases the risk of developing all grade with p less than 0.0001 and high grade HTN with p less than 0.0001.
Pathophysiology and Mechanism
The pathophysiology and mechanism for the difference in toxicity profile between two proteasomes is not clear as of yet. A possible explanation for higher toxicity related to Carf could be the irreversible nature of proteasome inhibition causing more significant myocyte toxicity. Cardiotoxicity of these novel agents is thought to be the result of modulation of endothelial nitric oxide synthase activity and nitric oxide levels by proteasome inhibition. Decreased eNOS activity leads to decrease in NO levels, which in turn leads to impaired vasodilation, hypertension, coronary artery disease and congestive heart failure. This modulation of eNOS is mediated by inhibition of chymotrypsin like activity of PIs in a dose dependent biphasic manner. It may be that irreversible nature of inhibition of chymotrypsin like activity by Carf leading to more sustained modulation in eNOS activity. This would require the cell to synthesize new proteasomes to recover their function which would take longer than the recovery of functionality from reversible inhibitors without the need for new protein synthesis. And thus irreversible inhibitors would provide a prolonged inhibition which could result in enhanced efficacy and potency but at the same time sustained oxidative stress and higher toxicity. Other explanation could be the possibility that RRMM patients would be heavily pretreated with other agents and would have a high likelihood of comorbidities. This seems less likely as the subgroup analysis shows that the cardiotoxicity was similar between studies with NDMM patients and those with RRMM patients. Moreover, there was no significant difference in high grade cardiotoxicity between Carf monotherapy and Carf based combination therapy. However, concomitant use of IMiDs did increase the incidence of cardiotoxicity significantly, which could be due to the known antiangiogenic effects of IMiDs leading to further endothelial dysfunction and increased platelet aggregation. Animal studies have also demonstrated that angiogenesis plays a key role in the normal adaptive response to a pressure load, and pressure overload in presence of antiangiogenic agents results in a reduction of myocardial capillary density, contractile dysfunction, myocardial fibrosis, and eventually decompensated CHF.
Dose Relationship
Some clinical trials showed higher ratio of cardiotoxicity with higher doses of Carf. However, this dose relationship with cardiotoxicity is not well established yet. The subgroup analysis also showed a similar insignificant ratio of cardiotoxicity with standard versus high dose of Carf.
Real World Implications
It is important to remember the cumulative incidences of side effects are from clinical trials where patients are healthy enough to enroll in a trial, which may not be the case in a real world setting. Moreover, cardiotoxicity in clinical trials is usually underreported. A retrospective multicenter observational study of 135 patients with RRMM, the reported incidence of Carf treatment related acute congestive heart failure was 9% with the majority being grade 3 or higher and requiring hospitalization. Similarly, in another case series of 60 MM patients, the reported incidence of cardiotoxicity was 12%. In the same analysis, the presence of any previously known cardiovascular disease was associated with an increased incidence of cardiac events at 23.5% versus 7% with p equals 0.07. As Carf is being increasingly used in real world settings and in clinical trials in combination with other agents, it is important for oncologists, cardiologist and primary care physicians to be aware of the risk of cardiotoxicity associated with Carf to monitor and treat it appropriately. Although it is recommended that patients receiving Carf should be closely monitored for cardiac complications, proper monitoring strategy is still a subject of debate and needs further research. As shown in the prospective ENDEAVOR study, serial echocardiograms have limited utility in the monitoring of the patients receiving this agent. Whether pro-BNP or cardiac enzymes could be used to monitor the cardiotoxicity associated with Carf is still unclear. Moreover, what factors predispose patients to develop cardiotoxicity from targeted agents is also unclear as traditional risk factors for cardiovascular diseases failed to show any association. Even though Carf seems to have a higher incidence of cardiotoxicity compared to bortezomib, the overall benefit of the drug still seems to outweigh the risk. Moreover, this toxicity seems largely reversible with prompt cessation of Carf and appropriate treatment of adverse event.
Study Limitations
There are a few limitations to this analysis. First, this analysis was based on the published data of the clinical trials, whereas an individual level data based analysis would have more detailed information on patient variables, such as comorbidities with baseline cardiac function, prior treatment exposure, and concomitant medications. Second, a few studies had to be excluded due to inadequate information on cardiotoxicity. Reporting of adverse events depends highly on the investigators, and could likely be confounded by other variables as well. Third, patients enrolled in trials usually have adequate organ function and are relatively healthier compared to the patients in common oncology practice. Fourth, the reporting of cardiotoxicity was highly variable among different studies, where some reported cardiotoxicity as a whole, such as cardiac disorders, whereas some reported cardiotoxicity separately in terms of congestive heart failure, arrhythmias, or cardiac arrest. Fifth, effect of heterogeneity needs to be taken into account for any meta-analysis. All the studies included here had the common objective of evaluating safety and efficacy of Carf, but the inclusion criteria were different among individual studies.
Conclusion
In summary, this meta-analysis demonstrates that Carf usage does significantly increase the risk of cardiotoxicity and HTN. Moreover, Carf seems to be associated with higher rates of cardiotoxicity than bortezomib. While dose relationship for this Carf toxicity cannot be established, concomitant IMiDs use seems to increase the likelihood of cardiotoxicity. Clinicians should be aware of this risk and provide close monitoring to patients receiving this novel agent.
Important Numerical Data and Study Parameters
The study presents several critical numerical findings and study parameters. A total of 29 prospective studies were analyzed enrolling 4164 patients. This includes 2036 patients from controlled trials with 1017 cases and 1019 controls. The median age of patients ranged between 58 and 72 years. The overall estimated cumulative incidence of all grade cardiotoxicity was 8.68% with 95% CI at 6.13% to 11.59% among 2660 patients from 23 studies. The cumulative incidence of high grade cardiotoxicity was 4.92% with 95% CI at 3.91% to 6.02% among 2808 patients from 28 trials. The incidence of mortality associated with cardiotoxic events was 0.91% with 95% CI at 0.49% to 1.43%.
For hypertension, the cumulative incidence of all grade HTN was 11.53% with 95% CI at 7.69% to 15.97% among 1905 patients from 14 trials. The cumulative incidence of high grade HTN was 4.60% with 95% CI at 2.42% to 7.33% among 1981 patients from 14 trials.
The estimated overall OR of all grade cardiotoxicity between Carf and control was 2.03 with 95% CI at 1.19 to 3.46 and p equals 0.010. The OR of high grade cardiotoxicity was 2.04 with 95% CI at 1.31 to 3.17 and p equals 0.002. The overall OR of all grade HTN was 2.93 with 95% CI at 2.21 to 3.89 and p less than 0.0001. The overall OR of high grade HTN was 3.33 with 95% CI at 1.98 to 5.60 and p less than 0.0001.
For subgroup analysis of cardiotoxicity, in NDMM patients, 9 trials included 76 events among 826 patients with incidence of 10.88% with 95% CI at 5.01% to 18.48%. In RRMM patients, 11 trials included 166 events among 1884 patients with incidence of 7.73% with 95% CI at 4.75% to 11.31% and p equals 0.38. For monotherapy, 9 trials included 101 events among 1426 patients with incidence of 5.77% with 95% CI at 2.95% to 9.34%. For combination therapy, 14 trials included 146 events among 1392 patients with incidence of 10.78% with 95% CI at 6.49% to 15.90% and p equals 0.06. For high dose Carf, 18 trials included 148 events among 1707 patients with incidence of 8.31% with 95% CI at 5.12% to 12.10%. For standard dose, 5 trials included 99 events among 953 patients with incidence of 9.97% with 95% CI at 6.18% to 14.49% and p equals 0.62. With concomitant IMiDs, 8 trials included 128 events among 1075 patients with incidence of 15.99% with 95% CI at 8.75% to 24.76%. Without IMiDs, 15 trials included 119 events among 1585 patients with incidence of 5.94% with 95% CI at 4.03% to 8.15% and p equals 0.006.
For high grade cardiotoxicity subgroup analysis, in NDMM patients, 10 trials included 37 events among 614 patients with incidence of 5.61% with 95% CI at 3.56% to 8.05%. In RRMM patients, 15 trials included 118 events among 2244 patients with incidence of 4.68% with 95% CI at 3.14% to 6.47% and p equals 0.46. For monotherapy, 13 trials included 83 events among 1786 patients with incidence of 4.07% with 95% CI at 2.43% to 6.04%. For combination therapy, 15 trials included 75 events among 1180 patients with incidence of 5.79% with 95% CI at 4.42% to 7.29% and p equals 0.10. For high dose, 20 trials included 89 events among 1595 patients with incidence of 4.90% with 95% CI at 3.68% to 6.27%. For standard dose, 8 trials included 69 events among 1213 patients with incidence of 5.02% with 95% CI at 3.24% to 7.12% and p equals 0.86. With concomitant IMiDs, 9 trials included 61 events among 863 patients with incidence of 6.45% with 95% CI at 4.71% to 8.41%. Without IMiDs, 19 trials included 97 events among 1945 patients with incidence of 4.34% with 95% CI at 3.26% to 5.54% and p equals 0.03.
Heterogeneity statistics showed I-squared equals 79.95% for all grade cardiotoxicity and I-squared equals 22.37% for high grade cardiotoxicity. Publication bias was assessed with Egger’s test showing p equals 0.200 for all grade and p equals 0.762 for high grade cardiotoxicity.